
There is a particular moment when the body shifts its breath without thinking. Someone sprints up a flight of stairs, chest heaving, shoulders pumping up and down with each desperate inhale. A person in the grip of panic gasps, feeling their collarbones rise and their shoulders hunch as their breathing becomes rapid and shallow. An anxious person sitting in a waiting room finds their upper chest rising and falling while their belly stays tight and still.
All of these are the raw expression of clavicular breathing. It is the breath of the body in extremis, the gasping, shallow, effortful pattern that emerges when demand exceeds the capacity of the diaphragm to cope. Yet this same breath also sits at the heart of an ancient yogic practice. In the tradition of pranayama, clavicular breathing is taught as the conscious, final layer of the three-part yogic breath a tool for awareness, for expanding lung capacity, for quieting the mind.
This is the central tension that makes clavicular breathing worth understanding. The same technique that serves as a deliberate, brief awareness practice in yoga is also flagged by respiratory physiotherapists, voice coaches, and speech therapists as an inefficient, often unhealthy default pattern. It is neither purely good nor purely bad. It is a real, named mechanism in the human breathing hierarchy that serves a clear short-term purpose and causes clear problems when it quietly becomes the norm.
This article explores what clavicular breathing is, how the body performs it, why yoga teaches it, why clinicians warn against it, and what it means for your health and voice if you find yourself doing it all day without realizing.
What Is Clavicular Breathing?
Clavicular breathing is a breathing pattern in which air is drawn mainly into the upper chest by raising the shoulders and collarbones the clavicles, those slender bones running horizontally across the front of your upper chest. In upper lobar breathing, clavicular breathing, or clavicle breathing, air is drawn predominantly into the chest by the raising of the shoulders and collarbone, and simultaneous contracting of the abdomen during inhalation.
The breath is most recognizable by what you can see and feel: the shoulders lift toward the ears, the collarbones rise, the chest inflates, and the belly draws in or stays pulled tight. The whole effort is visible and effortful.
You may also hear it called by other names. Upper chest breathing, upper lobar breathing, shallow breathing, chest breathing, and even thoracic breathing (though this term is sometimes used more broadly) all refer to variants of this pattern. Understanding the different names is useful because it helps you recognize clavicular breathing when you encounter it in yoga classes, medical literature, speech therapy texts, or fitness instruction.
Here is a key fact to grasp from the outset: a maximum amount of air can be drawn this way only for short periods of time, since it requires persistent effort. The reason is anatomical, and understanding it requires looking at how the body actually moves air in and out of the lungs.
The Anatomy and Mechanics

To understand why clavicular breathing is both possible and limited, it helps to know where it sits in the breathing hierarchy. Clavicular breathing is the final stage of total ribcage expansion. It occurs after the thoracic inhalation has been completed. In other words, it is not the first breath or the main breath. It is the reserve, the last increment of air the body pulls in when it has already expanded the lower ribs and needs more.
The mechanics are straightforward. In order to absorb a little more air into the lungs, the upper ribs and the collar bone are pulled upwards by the muscles of the neck, throat and sternum. This requires maximum expansion on inhalation and only the upper lobes of the lungs are ventilated. Note that phrasing: “only the upper lobes.” This is a crucial detail that explains why the body does not rely on this breath at rest.
The muscles that do this work are called accessory muscles, a telling name. They are secondary to the diaphragm, the large dome-shaped muscle beneath the lungs that should do most of the work during rest and calm breathing. The accessory muscles of inspiration include some specific players worth naming:
The sternocleidomastoid muscles originate from the manubrium of the sternum and sternal end of each clavicle, and allow them to elevate the sternum and clavicle, subsequently lifting the ribs during inhalation. Therefore, they are used as accessory muscles in ventilation. These muscles run from your breastbone and collarbone up to the sides of your skull, and you can feel them working if you place your fingers on the sides of your neck and take a big breath that lifts your shoulders.
The scalene muscles also play a role in inspiration. The scalenus anterior runs from the anterior tubercles of transverse processes of C3 to C6 vertebrae to the first rib, contributing to its elevation. The scalenus medius runs from the transverse processes to the first rib, also raising it. These are long, thin muscles that run from your cervical spine down to your ribs, and they too become active whenever you hoist your shoulders and upper chest to breathe.
What is remarkable is how much muscular effort goes into raising these bones. Compare this to how the diaphragm works. At rest, the diaphragm simply contracts and drops downward, like an elevator descending. This increases the volume of the thoracic cavity, the pressure inside drops, and air rushes into the lungs. It is efficient, quiet, and requires far less effort. Most of the oxygen exchange in the lungs happens in the lower lobes anyway, the part that opens up most when the diaphragm does its job.
The accessory muscles, by contrast, have to work hard to lift skeletal structures. They fatigue easily. And even when they succeed in lifting the ribs and collarbones, they are recruiting air into the upper lobes of the lungs, the region where less oxygen exchange actually occurs.
This is the functional anatomy of clavicular breathing: it is a method to add a little more air to the lungs, but at great muscular cost and with less efficient gas exchange. It is what the body resorts to when it needs more oxygen than the diaphragm and rib cage expansion can provide, such as during a sprint or an asthma attack. It is not what the body chooses for a day of quiet sitting.
Clavicular Breathing in Yoga: The Top of the Three-Part Breath
In the yogic tradition, clavicular breathing is rarely taught as the main event. Instead, it is the third and final layer of a systematic practice called the three-part breath, or in Sanskrit, Dirga Pranayama. Understanding this context is essential because it shows how yoga integrates clavicular breathing into a larger whole, and also how the tradition itself anticipates some of the concerns that modern clinicians raise.
The three-part breath includes the lower abdomen (abdominal breathing), the chest and ribs (thoracic breathing), and the upper chest or collarbone area (clavicular breathing), combined in a smooth, unobstructed flow. The student learns to breathe in layers, filling the body from bottom to top, and then exhaling in reverse. It is meditative and slow. The point is to expand the capacity of the lungs and to develop intimate awareness of how breathing moves through the entire torso.
What does this practice offer the practitioner? This breath technique aims to promote relaxation, increase lung capacity, and enhance awareness of the breath. Conscious deep breathing engages the parasympathetic nervous system, reducing stress and anxiety. In other words, the three-part breath is designed to calm the nervous system and to cultivate a felt sense of the body’s inner movements.
But here is where the yoga tradition’s own caution matters. In yoga, we only use clavicular breathing alone to create awareness, and afterwards combine it with thoracic and abdominal breathing to form yogic breathing. The teaching is explicit: clavicular breathing in isolation is a training tool, not an endpoint. Once the student understands what the upper lobes feel like when they fill with air, the practice moves on to the integrated breath where all three regions work together.
And the tradition also acknowledges the body’s own wisdom about when it reaches for this breath. This type of breathing is generally done in combination with thoracic breathing in periods of great stress such as strong physical exertion, or obstructive airways problems such as asthma or emphysema. Yoga texts recognize that the body naturally recruits clavicular breathing in emergencies. They teach it as a conscious choice, not as a default habit.
How to Practice Clavicular Breathing (Step by Step)
If you wish to experience clavicular breathing in the way yoga teaches it, here is the traditional method. This is distinct from the involuntary, unconscious clavicular breathing that happens during stress or exertion. This is deliberate, controlled, and brief.
Setup and groundwork. Begin by finding a disturbance-free place and sitting comfortably in Sukhasana (easy pose) or on a chair, focusing first on your natural breath, then practicing thoracic breathing. Silence or soft music is advisable. Your posture should be upright but relaxed. Let your awareness settle into the present moment.
The progression. Maintain unbroken awareness of the natural breath for some time, concentrating on the sides of the chest, then perform thoracic breathing for a few minutes. This is not rushing. You are priming the breath, moving the attention down into the middle and lower regions of the lungs, and preparing the body for the fine-tuning that comes next.
Now comes the active phase. Inhale fully, expanding the rib cage. When the ribs are fully expanded, inhale a little more until expansion is felt in the upper portion of the lungs around the base of the neck. You will feel a subtle shift as the focus moves upward. The shoulders and collar bone should also move up slightly, and this will take some effort. This is the moment of clavicular breathing. Feel the shoulders rise, the collarbones lift, the upper chest fill.
On the exhale, the sequence reverses. Exhale slowly, first releasing the lower neck and upper chest, then relaxing the rest of the rib cage back to its starting position. Let the shoulders drop. Let the collarbones settle. Complete the exhale before beginning again.
Completion. Continue for about five more breaths, observing the effect of this type of breathing. Then relax and return to observing the natural spontaneous breathing pattern before gently opening the eyes.
A practical tip: as you practice, place one hand on your upper chest and the other on your collarbones. Feeling the subtle lift of these bones with your own hands deepens the body awareness and gives you feedback that you are practicing the breath correctly. This dual attention to the physical sensation and to the inner experience is part of what makes the practice valuable in yoga.
The Benefits (When Used Intentionally and Briefly)
When practiced as yoga teaches, as a brief, conscious exercise within the three-part breath, clavicular breathing offers real benefits.
Interoceptive awareness. The practice sharpens interoception, the felt sense of subtle movement within your own body. Most people move through the day with little awareness of their collarbones or the upper reaches of their lungs. Practicing clavicular breathing brings attention to these usually-ignored regions. This expanded body awareness, cultivated over time, can carry over into daily life, making you more conscious of your posture, your breathing habits, and the subtle signals your body sends.
Lung capacity. Clavicular breathing, as the final layer of the three-part breath, contributes to fuller lung capacity. The technique aims to increase lung capacity and enhance awareness of the breath. Over time, regular practice of the three-part breath can improve your lungs’ ability to expand and your diaphragm’s ability to function efficiently across its full range.
Nervous system regulation. Conscious deep breathing engages the parasympathetic nervous system, reducing stress and anxiety. The practice is calming. The slowness, the attention, the full expansion and release all signal safety to the nervous system. Practitioners often report feeling more relaxed and centered after the three-part breath.
Functional reserve. On a purely physiological level, clavicular breathing reminds the body that it has a reserve gear. During intense physical activity, the body naturally calls upon these upper muscles to add extra air. Practicing clavicular breathing deliberately keeps this capacity available.
It is important to note that all of these benefits come from the practice as yoga teaches it: brief, deliberate, and integrated into a larger breath pattern. They do not apply to clavicular breathing as a default, unconscious habit that runs all day long. That is a different story entirely.
The Other Side: Clavicular Breathing as a Dysfunctional Default
Here is where the narrative shifts. What is useful for five conscious breaths or for a short sprint becomes a significant problem when it quietly becomes your resting breathing pattern.
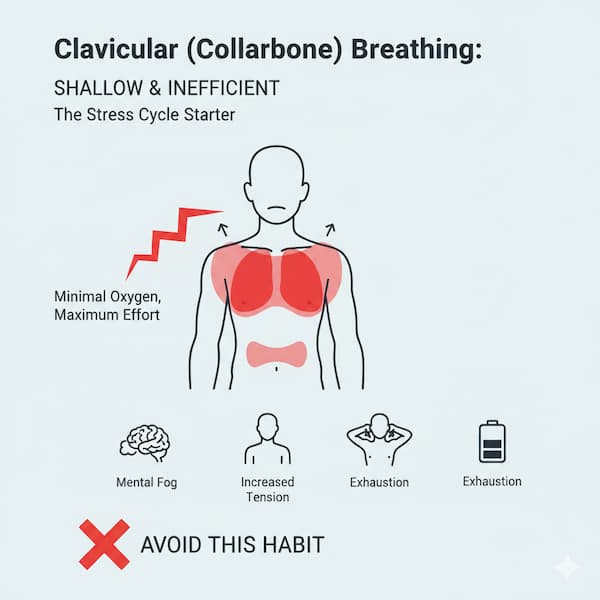
The efficiency problem. Oxygen exchange in the lungs is not equal throughout. The lower lobes of the lungs are where the greatest concentration of blood vessels passes through, which means the greatest opportunity for oxygen to transfer into the blood. The greatest amount of blood to collect oxygen occurs in the lowest area of the lungs, so shallow upper chest breathing means getting little oxygen, with poor transmission to the blood and little nourishment to the tissues.
When you breathe shallowly all day, exclusively in the upper lobes, you are starving the most efficient parts of your lungs of the work. Your blood does not pick up as much oxygen. Your tissues do not get as well nourished. You may not notice this on a moment-to-moment basis because the body is still getting by, but the cost accumulates.
How common is it? You might think that unconscious, all-day clavicular breathing is rare. It is not. Clinically this shows up as dysfunctional breathing, estimated at roughly 9 percent in the general adult population and much higher among patients seen for breathing complaints or asthma. One in eleven people around you is likely breathing this way without realizing it. Among people who have asthma or other breathing troubles, the proportion climbs much higher.
And here is the truly insidious part: most people who breathe shallowly do it throughout the day and are almost always unaware of the condition. People do not feel like they are breathing badly. They do not feel short of breath, because they are getting just enough air to get by. But the inefficiency is there, and it has consequences.
The stress loop. There is a bidirectional relationship between stress and clavicular breathing. When stress strikes a deadline looms, conflict erupts- the body perceives a threat, and the nervous system flips into a state of high alert. Part of that is a shift in breathing pattern. During anxiety or panic, rapid, shallow breathing shifts effort to the upper chest. The body is trying to be ready for action, and shallow, rapid breathing is part of that readiness.
But here is the problem: over time, if someone stays chronically stressed, or if they get stressed frequently, this upper-chest breathing pattern can stick around even when the acute stress has passed. The nervous system learns this pattern and defaults to it. And then the shallow breathing itself can reinforce the nervous system’s sense that there is a threat, because shallow breathing is the body’s crisis response. A vicious cycle develops.
A medical red flag. When clinicians and physiotherapists encounter reliance on accessory muscles, they pay attention. It is not always a sign of disease; plenty of people with healthy lungs slip into this breathing habit, but it is worth noting.
When the body starts to use additional muscles to help get the air it needs, it could be a sign you need medical attention. Reliance on accessory muscle breathing can appear in a wide range of conditions. Several conditions are marked by shallow breathing, including anxiety disorders, asthma, hyperventilation, pneumonia, pulmonary edema, and shock. In acute illness or during respiratory distress, the body summons these muscles out of desperation. When the same muscles are working hard at rest, it warrants investigation.
Clavicular Breathing in Singing and Speech
Voice teachers, coaches, and speech therapists have a word for clavicular breathing: avoid it.
Experts agree that high, or clavicular, breathing should be avoided for singing. This is not a suggestion or a preference. It is the consensus of the singing world, from classical opera to contemporary music. The reason is both mechanical and practical.
The mechanical problem. When you raise your shoulders and collarbones to breathe, you are doing work that does not translate into singing. The amount of muscle required to elevate the rib cage is extraordinarily fatiguing. Additionally, the speed with which the chest collapses after inhalation expels the air rapidly and with little control.
A singer needs control. The exhale should be smooth and sustainably regulated so that the breath supports the voice evenly across a phrase. But clavicular breathing does not permit this. This method generally limits the descent of the diaphragm and does not allow a singer to take a full, complete breath, leading the vocal folds to either fail to close completely, producing a breathy sound, or succumb to their biologically programmed response to act like a valve, closing too tightly and producing a tight or pinched sound.
In other words: a clavicular breather singing cannot maintain consistent pressure. Their sound will be unstable. They will run out of air mid-phrase. Their voice will lack power and control.
The tension problem. Beyond mechanics, there is the matter of tension. Raising the shoulders also requires a lot of energy, making clavicular breathing the least efficient way to breathe and creating a ton of muscle tension around the throat, which is important to keep as relaxed as possible.
Tension in the throat and neck is an enemy of good singing. The larynx needs to be free and mobile. The muscles around it need to be loose. When someone is breathing with their shoulders and neck muscles, those same muscles are tensed and cannot relax. The voice comes out restricted, tight, and effortful.
Implications for speech. The problem extends beyond singing to ordinary speaking. When it is time to speak, some people become tense and use shallow chest or clavicular breathing, which can lead to vocal cord tension, a quieter and less powerful sound, and over time, hoarseness or throat pain.
The mechanics are the same whether you are speaking or singing. When you chronically use accessory muscle breathing, your throat is chronically tense. Your vocal cords work harder. They do not vibrate efficiently. The result is a voice that sounds strained, lacks projection, and can develop problems like nodules or hoarseness if the pattern continues for years.
A note on nuance. The advice against clavicular breathing for singing is not absolute. Clavicular breathing fuels high-energy moments but can be hard to control. A trained singer might occasionally draw on a small amount of clavicular breathing to raise their larynx and add energy to a high note or an emotionally intense moment. But this is the exception, used sparingly and skillfully, not the foundation of the breathing technique.
Risks, Contraindications, and Who Should Be Cautious
If you are considering practicing clavicular breathing, or if you suspect you might be doing it unconsciously, there are specific cautions to observe.
Medical contraindications. If you have had recent surgery on your collarbone or ribs, or if you have a fractured collarbone, clavicular breathing is ill-advised. The movement of the structures involved could interfere with healing. People with fractured collar bones or any collar surgery should refrain from the practice.
If you have a frozen shoulder, clavicular breathing requires care. Students with frozen shoulders should be careful while doing the pose, and yoga teachers can guide them in placing their hands in front and elbows on the sides of the abdomen for shoulder support. The lifting motion might aggravate the condition, but modifications exist.
Some people are advised to avoid clavicular breathing entirely. People with vertigo and migraine should not do it. The theory is that the rapid pressure changes and the work of the neck muscles can trigger symptoms in these conditions.
Duration matters. When done for a longer duration, the oxygen supply becomes insufficient, which can increase stress and make the brain and body not function properly. In other words, if you practice clavicular breathing for more than a few minutes, or if you make it your default all day, you are going to underoxygenate your system. Your brain will not perform well. Your body will feel fatigued or anxious.
This is the key constraint that yoga texts emphasize. Prolonged practice can disrupt the body’s prana, so it should be practiced under teacher guidance until mastered. Prana is the yogic term for vital energy or life force. Disrupting prana in yogic terms means disrupting the smooth flow of breath and energy through the body. In modern terms, it means inefficient gas exchange and dysregulation of the nervous system.
The bottom line: Keep clavicular breathing brief, keep it conscious, and integrate it into the full three-part breath rather than isolating it for long stretches. If you are practicing it, do so under the guidance of a qualified yoga teacher who can ensure you are doing it in the context where it belongs. And if you suspect you are doing it all day without realizing, do not try to fix it on your own. Seek help from a respiratory physiotherapist or a breathing coach.
How to Tell If You Are a Chronic Clavicular Breather, and How to Shift
Most people who breathe shallowly do not know it. The breath feels normal to them because it is the only breath they have ever known. But there is a simple test you can do right now to check.
The two-hand test. Rest one hand on your tummy and one hand on your chest. Notice which moves: if it is the hand on your tummy, you are using your diaphragm to breathe. If it is the hand on your chest, you are using your accessory muscles.
Sit quietly for a moment and just notice. Do not try to change anything yet. Which hand is moving? If it is the chest hand that is moving while the belly stays still, you have likely developed a habit of upper chest breathing.
Visual and kinesthetic cues. Beyond the hand test, you might notice other signs. Your shoulders rise and fall with each breath. Your collarbones seem to move up as you inhale. Your belly stays pulled in or sucked in, rather than expanding. You might feel tension in your neck and shoulders that does not seem to go away. You might find that you sigh a lot, as if you are not getting enough air. You might feel breathless even at rest, or find yourself taking frequent deep breaths as if you need to reset.
The corrective direction: diaphragmatic breathing. If you have identified yourself as a chronic clavicular breather, the solution is to relearn diaphragmatic breathing. This is not complicated, but it does require attention and practice over weeks or months.
The goal is simple: reverse the pattern. Lead from the belly, not the chest. On the inhale, let your belly expand outward first. Your diaphragm is descending, the cavity of your chest is enlarging, and air flows in. Your chest will still move; that is normal, but it should be secondary, not primary.
Diaphragmatic breathing is deeper and more relaxed, giving your voice more support and letting you speak with less effort and no strain. Once you reestablish diaphragmatic breathing, the benefits emerge across multiple domains: your voice becomes stronger, your breathing becomes quieter and less visible, and your nervous system quiets down.
Some helpful practices. Yoga and breathing traditions use isolation drills to retrain the breath. If you are a chronic shallow breather, rather than trying to coordinate all three parts at once, you might practice abdominal breathing alone for several sessions. Focus entirely on the belly expanding and contracting while the chest stays relatively still. Once that is smooth, add thoracic breathing. Once both are integrated, then add the clavicular layer in the context of the three-part breath.
Some people find it helpful to lie on their back in a relaxed position (called Shavasana in yoga) and place a light weight on their belly, such as a book. As you breathe, let the weight rise and fall with your belly. This gives you feedback and makes the movement more obvious.
Others benefit from guided instruction. If you are trying to break a deeply ingrained habit, working with a respiratory physiotherapist, a yoga teacher trained in pranayama, or a breathing coach can accelerate the process.
Reassurance about chest movement. As you retrain your breathing, do not aim for a completely still chest. That is not the goal. Your diaphragm is descending, your lungs are pulled down and become enlarged, and the air rushes in to equalize the pressure. Just because you are using the diaphragm does not mean your chest will be still. Your chest will still rise and fall. The difference is that the movement originates from the diaphragm’s work, not from the accessory muscles’ effort. Your belly leads; your chest follows.
Quick FAQ
Is clavicular breathing bad?
Not inherently. It is inefficient as a constant default, but it is useful as a brief, intentional tool. When a sprinter finishes a race, clavicular breathing is the body’s appropriate response. When a yoga student practices it for five breaths in the context of a pranayama session, it is a valuable awareness exercise. The problem arises when it becomes your resting, unconscious pattern.
Is it the same as shallow breathing?
Clavicular breathing is the highest and shallowest form of the shallow breathing spectrum. Shallow breathing refers broadly to breathing that does not fully utilize the lungs. Thoracic (rib cage) breathing can be shallow but is more efficient than clavicular. Clavicular breathing is the most restricted and least efficient form.
Can clavicular breathing cause anxiety?
There is a bidirectional relationship. Anxiety causes clavicular breathing as part of the fight-or-flight response. But chronic clavicular breathing can also maintain or reinforce anxiety because the nervous system interprets shallow, rapid upper-chest breathing as a sign that danger is present. Breaking the clavicular breathing habit can help calm anxiety; addressing the underlying anxiety can help restore normal breathing.
Should singers ever use clavicular breathing?
Mostly no, with narrow exceptions. The classical consensus is that diaphragmatic breathing, complemented by thoracic expansion, is the correct technique. However, some modern styles or emotional moments might call for a brief touch of clavicular breathing to add energy or raise the larynx. This is the exception, not the rule, and requires training to use skillfully.
How long does it take to retrain my breathing?
It depends on how long you have been breathing this way. A habit that has been in place for years will take weeks or months to shift. However, awareness itself is the first step, and many people notice a difference after just a few days of focused attention and practice. Consistent work over four to eight weeks typically yields substantial change.
Should I see a doctor?
If you have shortness of breath at rest, if you feel chronically unable to take a full breath, if you have been experiencing anxiety or panic that correlates with your breathing, or if you have any underlying lung disease, respiratory condition, or chest pain, consulting with a healthcare provider is wise. A doctor can rule out medical conditions. If all is clear medically, a respiratory physiotherapist can help you retrain your breathing pattern.
Conclusion
Clavicular breathing stands at the intersection of yoga and respiratory physiology, of intention and habit, of ancient wisdom and modern clinical insight. It is a real, named layer of human breathing that evolved for a purpose. The body reaches for it during sprints, during asthma flares, during moments of high demand and low capacity. It is not wrong. It is not broken. It is adaptive.
Yet it is also a pattern that modern life can lock us into, especially when we are chronically stressed, sedentary, or digitally focused. A habit of shallow breathing becomes invisible, and the person breathing this way may never suspect that their fatigue, their anxiety, their vocal strain, or their general sense of being unable to “catch their breath” could stem from the way they breathe.
The yoga tradition understood this long before modern medicine quantified it. Teachers of pranayama included clavicular breathing in the three-part breath not as the destination but as one layer of a multifaceted practice. They taught it briefly, integrated it into a larger pattern, and warned students that prolonged practice would disrupt the prana. They knew the limits.
Here is what you can do, starting today:
First, notice. Place one hand on your belly and one on your chest. Which one moves? Just observe, without judgment. This is awareness. Awareness is the prerequisite for change.
Second, if needed, seek guidance. If you find that your chest hand is the one moving, and if you suspect you have been breathing this way for months or years, do not attempt to fix it alone. Work with a respiratory physiotherapist, a pranayama-trained yoga teacher, or a breathing coach. They can assess your pattern, rule out any underlying issues, and guide you through the retraining process.
Third, be patient. The breath is intimate and automatic. It lives below conscious awareness. Changing a breathing habit takes time, consistency, and self-compassion. You have been breathing this way long enough that it feels right to your body. It will take some time to feel different. That is normal.
And finally, remember this: the vast majority of people who breathe shallowly do not realize it, and the vast majority of people who retrain their breathing experience a palpable shift in how they feel. Better oxygenation, quieter anxiety, clearer thinking, and a stronger voice are not dreams. They are available to you through something as simple and profound as learning to breathe all the way down into your belly.
Your breath is always with you. It is worth getting right.
Sources
- Tummee.com (Clavicular Breathing)
- Clavicular Breathing Steps (Tummee.com)
- Clavicular Breathing Contraindications (Tummee.com)
- Three Part Breath Constructive Pose (Tummee.com)
- Yoga India Foundation
- Yogapoint
- Wikipedia (Shallow breathing)
- Kenhub
- HealthCentral
- Somatic Movement Center
- Leagrave Therapy
- Asthma and Respiratory Foundation NZ
- Voice Science
- Rider University (A Review of the Breathing Mechanism for Singing)
- Total Voice Studio
- Bax Music
- WELL SAID: Toronto Speech Therapy